* To learn more, download the full 2015 Economic Impact Study here: www.BenefitingAZ.org/EIS
Notwithstanding all of the foregoing—the jobs, the net economic benefits, the investment capital for tribes—it is important to underscore how much Indian reservation economies have to grow to reach parity with Arizona. In the latest data shown below in Figures 4 and 5, the gaps are large. Indian average income on the reservations was 40 percent of Arizona’s all races average and unemployment was more that twice Arizona’s average. What is more, the economic indicators shown in the figures correlate with a host of other indicators of quality of life.
Take a sampling of recent national health statistics. Indian adult diabetes prevalence was more than two-and-a-half times higher than that of Whites [1]. The tuberculosis rate for Indians nationwide was almost eight times higher [2]. American Indian infant mortality was 50% higher than the rate for non-Hispanic Whites [3]. And for a host of indicators, Indian health disparities in Arizona have been worse than for Indians nationwide [4].
Fig. 5
Per Capita Income in Arizona
2014 dollars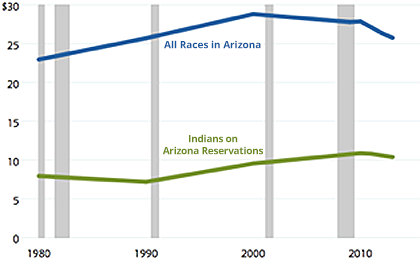
Fig. 5
Unemployment in Arizona
civilian labor force 16+ years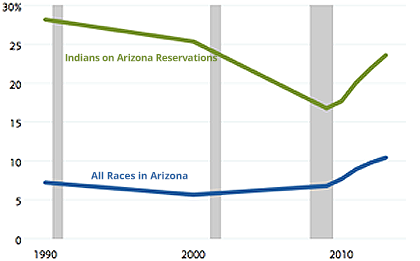
The federal government is not stepping into the breach. In 2003 the US Commission on Civil Rights found that “ federal funding directed to Native Americans…has not been sufficient to address the basic and very urgent needs of indigenous peoples.” Indian Health Service medical care expenditures per capita, for example, stood at half the level of expenditures on federal prisoners and a bit more than one-third of the average for all Americans [5]. In the years since that report, federal expenditures on Indian programs have not leapt upward to reverse a long-term relative decline [6].
Thus, not only is Indian gaming in Arizona providing substantial benefits to the Arizona economy as explained above, it helps tribes address serious accumulated complications from poverty—social conditions that neither federal or state policy adequately address. That work must continue because the unmet need remains large.
Footnotes:
- Barnes PM, Adams PF, Powell-Griner E. Health characteristics of the American Indian or Alaska Native adult population: United States, 2004–2008. National Health Statistics Reports. 2009;: 1–23. Available: http://www.cdc.gov/nchs/data/nhsr/nhsr020.pdf
- US Department of Health Human Services, Office of Minority Health. Profile: American Indian/Alaska Native. In: minorityhealth.hhs.gov [Internet]. Washington, DC; 19 Feb 2015 [cited 23 Sep 2015]. Available: http://www.minorityhealth.hhs.gov/omh/browse.aspx?lvl=3&lvlid=62
- Mathews TJ, MacDorman MF, Thoma ME. Infant mortality statistics from the 2013 period linked birth/infant death data set. National Vital Statistics Reports. 2015;64: 1–30. Available: http://www.cdc.gov/nchs/data/nvsr/nvsr64/nvsr64_09.pdf
- Indian Health Service. Regional differences in Indian health, 2002-3. Washington, DC: US Department of Health and Human Services, Indian Health Service; 2007.
- US Commission on Civil Rights. A quiet crisis: federal funding and unmet needs in Indian Country. Washington, DC: US Commission on Civil Rights; 2003.
- Walke R. Indian-related federal spending trends, FY 1975–2001, US Congressional Research Service memorandum, March 1, 2000. Report of the Committee on the Budget, United States Senate to accompany S Con Res 101 together with additional and minority views, Senate Report 106-251. 2000. pp. 199–250.